Vulvodynia: Persistent vulvar pain
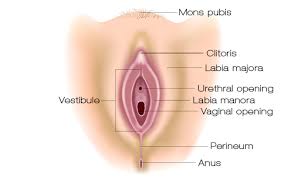
We have discussed persistent pain. Now I would like to talk about pelvic pain conditions. One painful condition is called Vulvodynia. (Vul – Vo – Din – Ee – Uh) Vulvodynia actually means pain in the vulva. The vulva is the external genitalia in women. Pain is often aching, burning pain. It can be one sided, or throughout the area.
The pain in vulvodynia is not caused by a clinical disease. Some common treatable disorders that might cause pain in the vulva are (not limited to) yeast infections, dermatological conditions (lichen sclerosis, dermatitis), hormonal changes, neuralgias. These can also cause persistent pain in the vulvo-vaginal area, but are not defined as vulvodynia.
The cause of vulvodynia remains under study. To date, we don’t have a solid answer. There are studies that have correlated genetic, immunological, hormonal, nerve and developmental factors as possible sources. Most likely it is a combination of factors: environmental, experiential and genetic/developmental that culminate toward a persistent pain state. These multiple factors require a group of providers who understand vulvodynia, persistent pain AND the other vulvo-vaginal conditions that ARE NOT vulvodynia.
There are two primary types of vulvodynia. Provoked vulvodynia (PVD) is more localized pain that is sharp and comes on with pressure, touch in the area. PVD is the most common type of vulvodynia. Generalized vulvodynia (GVD) is pain throughout the vulvar area that is constant or mostly constant and may worsen with pressure/touch, and does not go away. GVD is often described as a burning, achy pain.
The Numbers
The it estimated that anywhere from 1% up to 28% of women have vulvodynia. It is often under-reported. Many women in the United States may experience persistent vulvar pain during their lifetime. And even if only a small percentage of these women actually have vulvodynia, this is still a very large number. What is worse, at least 30% will suffer without seeking medical care. And many who do seek medical care do not find proper treatment for months or years. This post is meant to be a helpful tool. To help with what to ask your doctor, and help you to advocate for yourself.
Where to begin
If you have pain in your vulva and it has persisted longer than 3 months, see your gynecologist. Ask them to rule out infections, dermatological conditions, hormonal concerns. Ask them what they know about vulvo-vaginal pain disorders. Don’t feel like you are being pushy. It is your body, your health, you can ask these questions. If your MD seems defensive or angry, or tells you it’s in your head…find a new one.
Find a pelvic floor physical therapist. PT’s also have varied experience and knowledge, so ask your PT the same questions. If they don’t know, ask them to help you find the answers! A pelvic floor PT will help you manage not only the muscles and nerves of the pelvis, but should be discussing with you the nutritional, environmental, emotional, activity and sleep factors that can help you heal. This is a big part of caring for persistent pain conditions. If your therapist isn’t taking time to educate you about chronic pain, they should. Understanding the brain’s role in pain is a huge part of healing.
Another provider that should be a part of your treatment team, is a mental health provider, who is also familiar with pelvic pain conditions. Many women who struggle with pelvic pain feel ashamed, embarrassed and this lends itself to anxiety and depression. It is important that you are addressing the physical and emotional components of your pain.
Assessment of vulvar pain
It is very important that a thorough assessment is taken. This means a very in-depth medical history, especially medications. There are some medications that have been associated with patient report of vulvodynia. So it is important to consider medication use and timeline of pain presentation.
Antibiotics are commonly prescribed in women. Antibiotics do not directly cause genital pain, but long-term use can cause chronic yeast infections. This has been associated with vulvodynia. Hormonal contraceptives are another common medication used chronically by women. Studies suggest that oral contraceptives contribute to vulvodynia. because they decrease testosterone levels, which are important for vulvar health. Many women use prescription medications for anxiety and depression. These medications can contribute to painful intercourse due to their effects on vaginal lubrication.
A thorough assessment of your vulvar area and a vaginal exam of the pelvic floor muscles is also necessary. A pelvic floor PT will examine your vulvar tissues, for coloring, lubrication, and structures to make sure there aren’t any signs of clinical disease, again we want to rule out anything else. They will also do what is called a Qtip test, which is very important in vulvodynia. This is what will help to diagnose vulvodynia, and determine if it is localized to one area or if it is more diffuse, throughout the whole vulva. Last, they will do a vaginal exam, which allows for a baseline of the pelvic floor muscle function.
Treatment
Physical Therapy is an important part of the treatment plan. After assessing the tissues, and muscles your therapist should develop a plan of care to address your specific concerns. With a focus on muscle lengthening and relaxation, and eventually adding in strength, PT can provide great results. A pelvic physical therapist will educate you regarding products that might be harmful to your tissues, and good hygiene practices to mitigate irritation and pain.
Psychological treatment with a mental health provider is another important part of your team. The emotional toll that vulvodynia can take on a person is huge. The number of providers you often see without good answers, or worse, made to feel your pain is in your head can do a number on anyone. It is important to address the depression and anxiety that can often be associated with vulvodynia.
There are many topical medications (analgesics, steroids, hormones) that have been used to treat vulvodynia. Some of them can be helpful, and some can cause dermatitis in the vulvar tissues, which clearly needs to be avoided if you have vulvodynia. It is important that you communicate with your physician if your pain, burning, itching symptoms arise or increase after a new medication. That is not what is intended. It is very important your physician is familiar with all the options for treating vulvodynia.
Antidepressants may be prescribed for vulvodynia, as they are commonly used in the treatment of many chronic pain conditions. Some commonly prescribed are Tri-cyclic Antidepressants like amitriptyline, nortriptyline, and desipramine. These medications quiet nerves that cause the pain sensations. The dosages of these for vulvodynia are usually less than those used for depression.
Other antidepressants (SSRI’s), have been used for pain control in vulvodynia, but in general, they have not been shown to be effective for pain relief in the majority of women. However, there is some promise in taking SNRI’s (selective norepinephrine reuptake inhibitors) for treating vulvodynia.
Some Neuromodulators (Gabpentin and Neurontin) have been used to treat vulvodynia, and these tend to have fewer side effects than the tricyclic antidepressants.
All medication questions should be discussed with your doctor. This is just a short list of common meds that may be suggested.
A physical therapist with experience with vulvodynia can help you find a doctor, mental health provider and any alternative therapy providers that may be helpful to you. We offer a free 15 minute phone consultation to answer questions and make sure our practice is the right fit for you. Click here to schedule!
–Sarah Dominguez, PT, MSPT, WCS, CLT, CMTPT
References:
https://www.sophiebergeron.ca/images/publications/Goldstein_2016_Vulvodynia.pdf
https://www.tandfonline.com/doi/abs/10.1080/713846809
https://escholarship.org/uc/item/5b74k0n3
https://www.isswsh.org/images/PDF/Consensus_Terminology_of_Vulvar_Pain.pdf
Disclaimer: This blog is here for your help. It is the opinion of a Licensed Physical Therapist. If you experience the symptoms addressed you should seek the help of a medical professional who can diagnose and develop a treatment plan that is individualized for you.
Related Posts
The Surprising Connection Between Low Back Pain and Pelvic Floor Dysfunction in Women
Why it might be more than your back Low back pain is one of the most common reasons women seek…
Pelvic Pain and your Low Back: You can’t treat one without the other
Pelvic pain can affect nearly every part of daily life. Sitting, walking, exercising, and even sleeping may become difficult. Many…
Back Fusion Recovery: Why Physical Therapy Can Make or Break Your Results
Recovering from sacroiliac joint (SIJ) fusion or lumbar fusion surgery is not just about letting bones heal. It is also…