What Most Women (and Even Providers) Miss About Back Pain After Childbirth
Low back pain and pelvic floor problems are both common in women, especially after childbirth. The levator ani defect—a tear in one of the main pelvic floor muscles—can have a connection with low back pain. Low back pain is more closely related to poor pelvic floor muscle coordination than to the structural tear itself. In other words, it is usually the way the muscles function after injury, not the injury alone, that contributes to back pain.
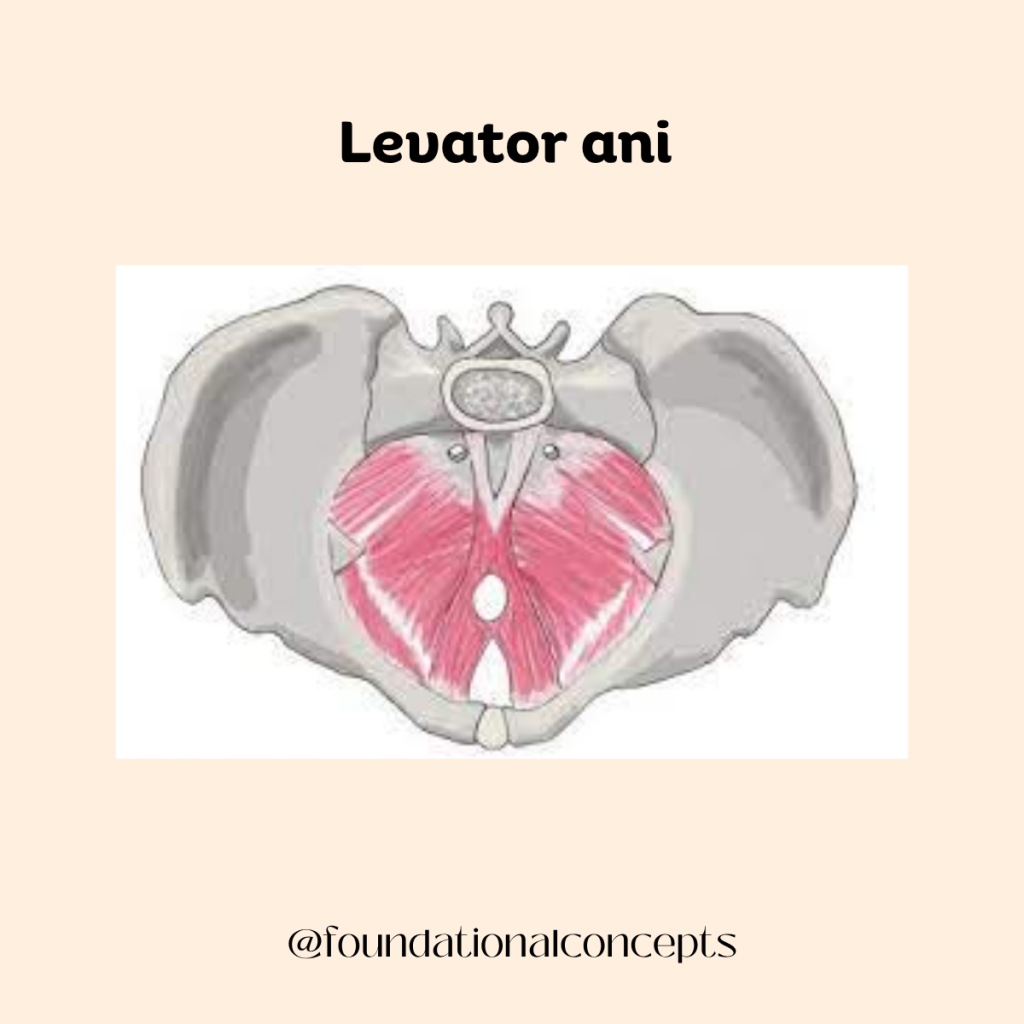
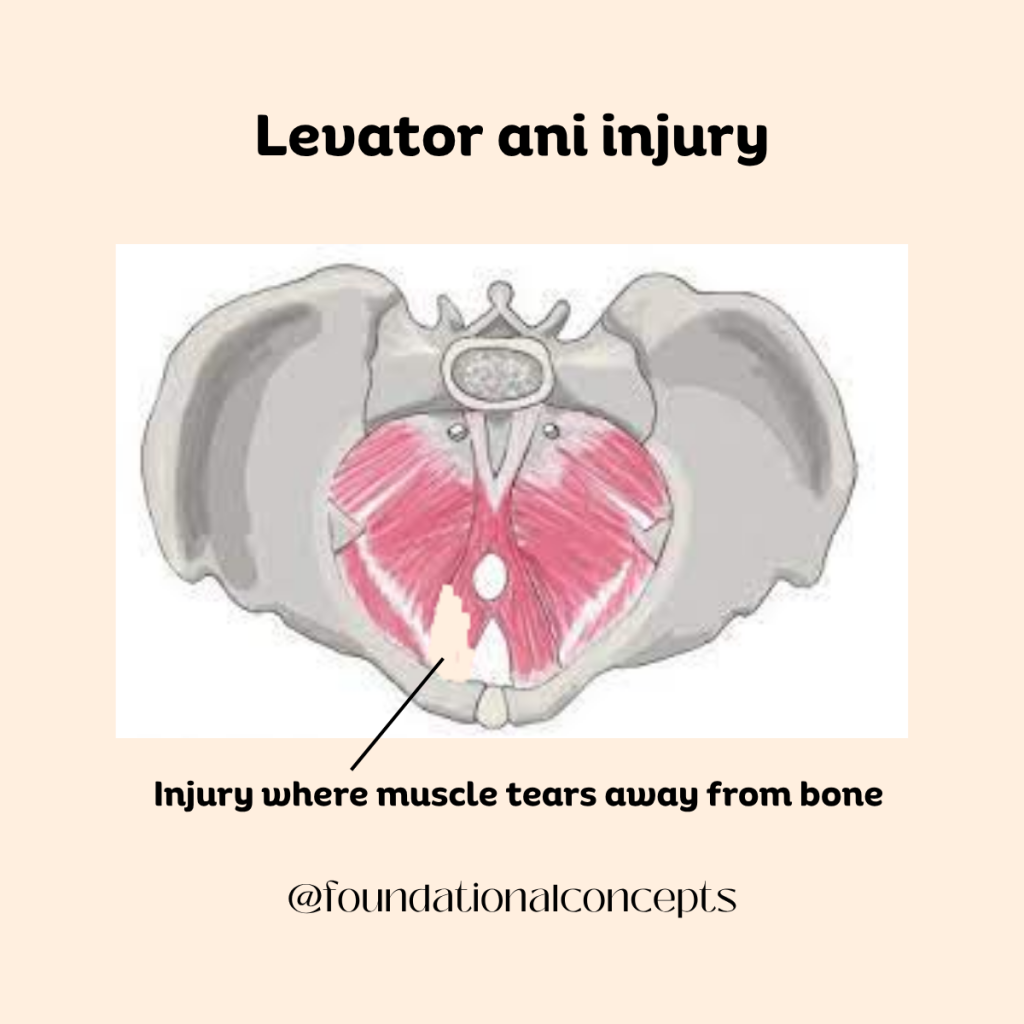
The levator ani is a group of muscles that forms the main support of the pelvic floor. These muscles support the bladder, uterus, and rectum, help control urination and bowel movements, and work together with the deep abdominal and back muscles to stabilize the spine. During vaginal childbirth, part of the levator ani muscle can detach from the pelvic bone. This is called a levator ani avulsion or defect. Levator defects are strongly associated with pelvic organ prolapse, a condition in which the pelvic organs drop downward and press into the vaginal wall. While this structural injury can affect pelvic support, it does not automatically lead to low back pain.
Research shows that poor pelvic floor muscle coordination is strongly associated with non-specific low back pain. Studies have found that decreased pelvic floor muscle coordination is an independent predictor of disability in women with back pain, even when age, body mass index, and childbirth history are taken into account. The pelvic floor is part of the “core” system, which also includes the diaphragm, deep abdominal muscles, and small stabilizing muscles in the spine. These muscles work together to control pressure in the abdomen and provide stability to the lower back. If the pelvic floor is poorly coordinated, other muscles may compensate. This can change movement patterns, increase strain on the lumbar spine, and contribute to ongoing pain.
Pelvic floor dysfunction is highly prevalent in women with lumbopelvic pain. In one cross-sectional study, the vast majority of women presenting with low back or pelvic girdle pain had some form of pelvic floor dysfunction. Many had muscle tenderness, weakness, or even pelvic organ prolapse. Women who had both low back pain and pelvic girdle pain tended to report greater disability and more severe pelvic floor symptoms. These findings suggest that pelvic floor dysfunction is often part of the broader clinical picture in women with back pain.
The nervous system also plays a role in this connection. A concept known as viscerosomatic convergence helps explain how pelvic problems can influence the low back. When there is ongoing irritation or dysfunction in pelvic structures, the nervous system can increase muscle tension in nearby areas. This may lead to muscle guarding, trigger points, and referred pain into the hips, buttocks, and lumbar region. At the same time, chronic low back pain can alter how pelvic floor muscles activate and coordinate. This creates a cycle in which dysfunction in one area reinforces dysfunction in the other.
Because of this overlap, internal vaginal pelvic floor examination may be appropriate in some women who present with persistent low back, hip, or pelvic girdle pain, even if they do not report vaginal symptoms. Research has shown that a large percentage of women with external lumbopelvic pain have internal pelvic floor muscle tenderness on examination. Identifying these issues can help guide more targeted treatment.
Even though pelvic floor muscle training cannot fix the tear itself, it can still provide important benefits. Strengthening the remaining intact muscle fibers can improve overall pelvic floor function. Research shows that pelvic floor muscle training significantly reduces low back pain intensity, especially when programs last longer than eight to twelve weeks. Adding pelvic floor exercises to general core or stabilization programs often results in greater pain reduction than exercise alone. Women with chronic non-specific low back pain who complete structured pelvic floor–focused programs show improvements in pain, disability, pelvic floor strength, and deep abdominal muscle activation. Postpartum women also benefit from home-based programs that combine stabilization and pelvic floor exercises.
In women with levator defects, pelvic floor muscle training can increase muscle strength and improve contraction ability even when the structural injury remains. Training has been shown to reduce the size of the levator hiatus and improve the shape of the pelvic floor opening, which is associated with better muscle force and reduced incontinence severity. Importantly, the effectiveness of pelvic floor muscle training for pelvic organ prolapse does not appear to depend on whether a levator defect is present. Large clinical trials have demonstrated that individualized pelvic floor muscle training reduces prolapse symptoms and improves quality of life, with benefits lasting at least one year.
Overall, the evidence suggests that levator ani defects themselves are not the direct cause of low back pain. Instead, pelvic floor muscle weakness and dysfunction are key contributors. Many women with back pain have unrecognized pelvic floor issues that may be influencing their symptoms. Pelvic floor physical therapy should be considered a first-line conservative treatment for women with low back pain and pelvic floor dysfunction because it addresses functional weakness, improves coordination, and reduces pain, even though it cannot repair structural tears. Programs are most effective when supervised, progressive, and continued for at least twelve weeks.
Understanding the difference between structural damage and muscle function is essential. Imaging findings alone do not determine pain. What matters more is how well the muscles work together to support the spine and pelvis. By focusing on restoring strength, coordination, and proper movement patterns, many women can experience meaningful improvements in both pelvic floor symptoms and low back pain, even in the presence of a levator ani defect.
Disclaimer: This blog is here for your help. It is the opinion of a Licensed Physical Therapist. If you experience the symptoms addressed you should seek the help of a medical professional who can diagnose and develop a treatment plan that is individualized for you.
Related Posts
Is Your Child Afraid to Poop? What Parents Need to Know
Constipation in children is a very common problem, and it can be stressful for both kids and their families. When a…
The Surprising Reason Your Knee Pain Won’t Go Away
Pain in the knee does not always start in the knee. Sometimes the real source of the problem is higher…
Pre-habilitation for Prostate Surgery
Radical prostatectomy is a common surgery used to treat prostate cancer. While it can be very effective at removing cancer,…