
Constipation after Delivery: Why your Abdominal Wall might be Contributing to the Issue.
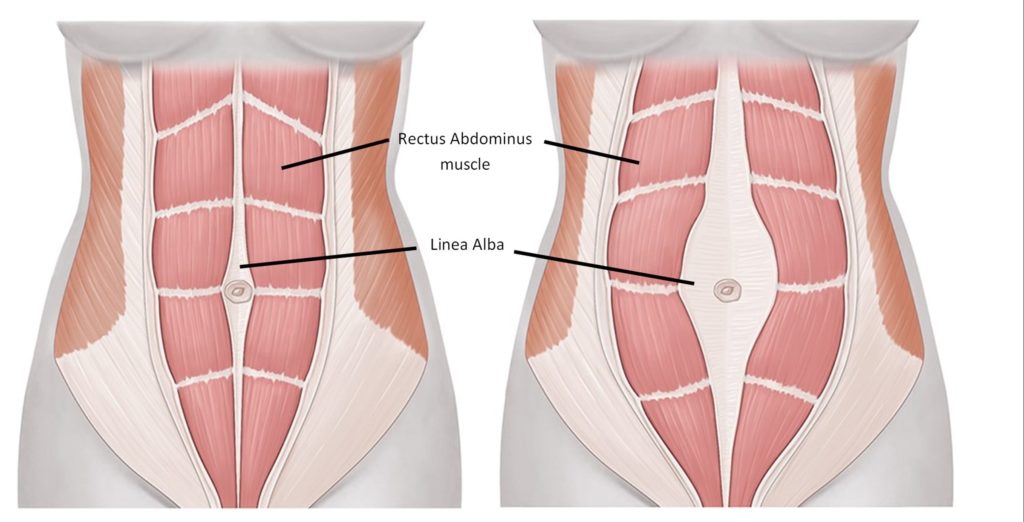
Diastasis rectus abdominis (DRA) is a common condition in women after pregnancy. It happens when the two sides of the main abdominal muscle, called the rectus abdominis, separate along the midline of the belly. This separation stretches the connective tissue between the muscles and can lead to weakness in the abdominal wall. Many people think of DRA as a cosmetic issue. However, research now shows that it may also affect how the body works, including bowel function. One important concern is constipation.
Constipation is common after childbirth. Hormonal changes, pelvic floor strain, pain, stress, and changes in routine can all slow bowel movements. For some women, DRA may also play a role. Recent research suggests that about half of postpartum women with DRA report constipation. In one prospective study published in the journal Aesthetic Plastic Surgery, about 50% of women with DRA said they struggled with constipation before surgery. After surgical correction of the abdominal separation, constipation dropped to 15%. Even more striking, nearly 97.5% of patients reported improvement in gastrointestinal symptoms overall. These findings suggest a strong link between DRA and bowel problems in postpartum women.
At first glance, this makes sense. The abdominal muscles play an important role in bowel movements. To pass stool, the body must increase pressure inside the abdomen. This is called intra-abdominal pressure. The abdominal muscles contract while the pelvic floor muscles relax. When this process is well coordinated, stool can pass smoothly. But when abdominal muscles are weak or separated, pressure generation may be less effective. This can make bowel movements harder.
Another key concept is abdomino-anal coordination. Research in Clinical Gastroenterology and Hepatology explains that proper defecation requires coordination between abdominal muscles and the anal sphincter. In people with defecatory disorders, the abdominal muscles may not activate properly. The pelvic floor may tighten instead of relax. This is called abdomino-anal dyscoordination. If DRA weakens the front of the abdominal wall, it could make this coordination even harder.
Experts now recommend a combined rehabilitation strategy for women with DRA and constipation. Instead of focusing on one muscle group, therapy targets the entire system. This includes deep abdominal muscles, surface abdominal muscles, pelvic floor muscles, and breathing patterns.
Core exercise programs are a key part of treatment. Studies show that programs combining deep muscle training, such as the transversus abdominis, with superficial muscles like the rectus abdominis and obliques work better than isolated exercises. Adding breathing exercises or pelvic floor training improves results. These combined programs reduce the distance between abdominal muscles and improve trunk strength. Stronger muscles can help generate the pressure needed for bowel movements.
Pelvic floor therapy is also important. Rehabilitative ultrasound-guided therapy helps patients learn how to coordinate muscle activity during defecation. With visual feedback, patients can see whether they are tightening or relaxing the correct muscles. This method is strongly supported for treating defecatory dysfunction. Programs that combine pelvic floor exercises, physical activity, and lifestyle education have shown improvements in constipation symptoms and quality of life.
Breathing exercises, especially diaphragmatic breathing, also help. The diaphragm works together with abdominal muscles to control pressure in the abdomen. Learning how to breathe deeply and coordinate breath with muscle contraction can improve bowel frequency. Abdominal massage has also shown meaningful benefits. In randomized trials, massage improved constipation severity, increased bowel frequency, and enhanced quality of life. Some programs also include abdominal supports or corsets. When used together with exercise, they may improve outcomes more than either approach alone.
For patients with both DRA and constipation, an integrated approach is often best. This may include progressive core stabilization exercises, pelvic floor training with rehabilitative ultrasound imaging, diaphragmatic breathing, abdominal massage, and simple lifestyle changes. Lifestyle strategies can include timed bathroom visits, proper hydration, fiber intake, and elevating the feet on a small stool during bowel movements to improve posture.
In summary, growing evidence suggests that DRA may be associated with constipation in postpartum women. Combined abdominal and pelvic floor rehabilitation offers a promising, non-surgical approach through improved abdominal wall strength and improved pressure generation for improved bowel movements.
Disclaimer: This blog is here for your help. It is the opinion of a Licensed Physical Therapist. If you experience the symptoms addressed you should seek the help of a medical professional who can diagnose and develop a treatment plan that is individualized for you.
Related Posts

Reclaim Your Run: Supporting Your Body After Pregnancy
Returning to running after pregnancy requires patience, preparation, and guidance. Pregnancy and delivery bring remarkable changes to the body, particularly…
Perineal Tears during vaginal delivery: What. Why. and How to reduce risk and severity.
Vaginal birth is an incredible and empowering experience, but it can also come with challenges—including perineal tearing. While some degree…

Pudendal Nerve Injuries During Childbirth
Childbirth can bring significant physical changes and challenges. Among them, pelvic nerve injuries—especially those affecting the pudendal nerve—can cause lasting…